Basic GI Anatomy and Physiology
Anatomy of the Digestive Tract (from Wikipedia)
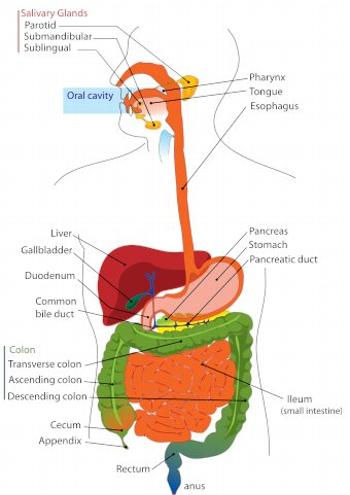
Anatomy of the Digestive Tract
This anatomical drawing shows the major organs of the GI tract. An important organ which is not identified is the midsection of the small intestine, the jejunum, which is downstream from the duodenum (section of small intestine as it leaves the stomach) and upstream of the ileum (section of small intestine entering the colon). The colon is also called the large intestine.
The esophagus conveys swallowed solids and liquids to the stomach. The stomach secretes digestive acid and enzymes which are mixed into food matter by the stomach's grinding function. The stomach's processed matter is then delivered to the duodenum, where bile and pancreatic fluids are added.
Absorption of nutrients (fat, protein, carbohydrate, vitamins, minerals) occurs in the small intestine. Absorption of water and electrolytes occurs in the large intestine (colon).
Index of Information About Specific Diseases, Conditions or Treatments
A
B
- Barrett's esophagus - Monitoring and treatment from UpToDate
- Breath Tests
- Fructose Malabsorption
- Lactose Intolerance
- Small Intestine Bacterial Overgrowth (SIBO)
- Books of Interest Page
C
- Calcium and vitamin D for bone health from UpToDate
- Celiac disease (sprue)
- Celiac disease from UpToDate
- Celiac Disease Foundation
- Celiac Sprue Association
- Prometheus Celiac Plus
- Publications: Gluten-Free Living available in Durango at Nature's Oasis
- Sources for uncontaminated oats: Gluten Free Oats | Cream Hill | Bob's Red Mill
- Cirrhosis from UpToDate
- Clostridium difficile (Antibiotic-associated diarrhea) from UpToDate
- Collagenous colitis from the National Digestive Diseases Information Clearinghouse
- Colon polyps from UpToDate
- Colon cancer
- What You Need To Know About Cancer of the Colon and Rectum from the National Cancer Institute
- Colorectal cancer screening: questions and answers from the National Cancer Institute
- Screening for colon cancer from UpToDate
- Treatment of rectal cancer from UpToDate
- Treatment of colon cancer from UpToDate
- Hereditary cancer testing at Myriad Tests
- Constipation in adults from UpToDate
- Crohn's disease
D
- Diarrhea
- Dictionary of Cancer Terms from the National Cancer Institute
- Diet and health from UpToDate
- Diet and FODMAPs (see FODMAPs below)
- Fiber Intake Calculator
- Fiber recommendations
- Ketogenic Diet from Diet Doctor
- 21 Day Sugar Detox – See our Books of Interest Page for a reading recommendation
- Virta Health - Reverse type 2 diabetes and pre-diabetes
- Diverticulosis and diverticulitis - Diverticular disease from UpToDate
- Dyspepsia from UpToDate
- Iberogast is available at Seacoast Vitamins
E
- Eosinophilic esophagitis from the American Partnership For Eosinophilic Disorders
- Eosinophilic esophagitis from the Children's Digestive Health and Nutrition Foundation and The International Gastrointestinal Eosinophil Researchers (TIGER)
F
- Fecal incontinence from UpToDate
- Fiber recommendations
- FODMAPs
- Low FODMAPs Diet from the Gastroenterological Association of Australia
- Low FODMAPs Diet from Shepherd Works
- Detailed review: Gibson PR, Shepherd SJ. Evidence-based dietary management of functional gastrointestinal symptoms: The FODMAP approach. Journal of Gastroenterology and Hepatology. 2010.
G
- Gallstones from UpToDate
- Gas and bloating from UpToDate
- Gastroesophageal reflux disease in adults (GERD) from UpToDate
- Bedge Foam bed wedge (recent searches suggest that this product, which helped many patients, is no longer available)
- MedCline Foam bed wedge (designed for side sleepers)
- Proton Pump Inhibitor (PPI) medications (Prilosec®, Prevacid®, Aciphex®, Protonix®, Nexium® and generics)
- Gilbert's syndrome from UpToDate
H
- Helicobacter pylori infection and treatment from UpToDate
- Hemochromatosis from UpToDate
- Hepatitis from UpToDate:
- Hemorrhoids from UpToDate
- Hemorrhoid CRH O'Regan System
- Hemorrhoid treatments that can be performed during colonoscopy
- Hemorrhoid treatment aftercare
- Hiatal hernia from MedicineNet.com
L
- Lymphangiectasia, intestinal from eMedicine
- Lymphocytic colitis from the National Digestive Diseases Information Clearinghouse
O
- Obesity from UpToDate:
P
- Pancreatitis from UpToDate:
- Peptic ulcers from UpToDate:
- Probiotics
- Probiotics from the AGA Patient Center - Choosing the right Probiotic
- Align® Bifidobacter infantis 35624
- P3-OM from Bio-optimizers
- Culturelle® Lactobacillus GG
- Florastor® Saccharomyces boulardii
- Pendulum - The only probiotic clinically shown to lower blood glucose spikes
- Phillip's Colon Health® Lactobacillus acidophilus, Bifidobacterium bifidum, Bifidobacteria longum
- VSL#3® Bifidobacterium breve, Bifidobacterium longum, Bifidobacterium infantis, Lactobacillus acidophilus, Lactobacillus plantarum, Lactobacillus paracasei, Lactobacillus bulgaricus, Streptococcus thermophilus
- Proton Pump Inhibitors
S
- Small Intestine Bacterial Overgrowth (SIBO) | Guidelines | Breath Testing
U
Educational Sites of Interest
- American Gastroenterological Association - Patient Center
- American Liver Foundation
- Association of Cancer Online Resources
- Clinical Trials
- Crohn's and Colitis Foundation of America
- Lab Tests Online
- Mayo Clinic Health Site
- National Center for Complementary and Alternative Medicine
- National Digestive Disease Information Clearinghouse
- New York Times Health
- PubMed National Library of Medicine
- Radiology Info - ACR & RSNA
- UpToDate for Patients
- WebMD
- Your Disease Risk
- Colorado Advance Directives - Living Wills
Diagnostic Tests and Procedures
Breath Tests
Breath testing relies on the detection of substances resulting from the body's breakdown of an ingested test solution in your exhaled breath. Breath testing is useful as a noninvasive tool for diagnosing Helicobacter pylori infection of the stomach, small bowel bacterial overgrowth (SIBO), lactose intolerance and fructose malabsorption.
Breath tests are administered through our office. Contact Metabolic Solutions for information regarding charges and billing.
Types of Breath Tests We Offer:
- Urea Breath Test (H. pylori) - Preparation: Avoid antibiotics, bismuth, and proton pump inhibitors for 2 weeks before test. Fast for 1 hour before test.
- Bacterial Overgrowth (SIBO) Test - Lactulose breath hydrogen-methane test. Requires 12-hour overnight fast and specific dietary restrictions the day before.
- Lactose Intolerance Test - 12-hour overnight fast required. Avoid antibiotics for 2 weeks before test.
- Fructose Malabsorption Test - 12-hour overnight fast required. Avoid high-fiber foods day before test.
Capsule Endoscopy ("Pill Camera")

PillCam SB Image of Normal Small Intestine
Capsule endoscopy devices
Capsule endoscopy is a technique that allows gastroenterologists to directly view the entire length of small intestine (duodenum, jejunum and ileum), which lies too far downstream to reach through the mouth with routine upper endoscopy, and too far upstream to reach during colonoscopy.
Used for: Evaluation of bleeding, anemia, diarrhea, suspected Crohn's disease, and small intestine tumors.
Risk: Capsule "retention" (becoming stuck) occurs in 0-13% of tests depending on patient history. Highest risk in patients with known Crohn's disease, NSAID use, prior surgery or radiation.
Esophageal Function Tests
Esophageal Manometry (High Resolution with Impedance)
Performed at Mercy Regional Medical Center
Used to evaluate swallowing problems (dysphagia), chest pain suspected to be due to esophageal disease, and to assist in pH probe placement or preoperative assessment for anti-reflux surgery. No sedation used. A soft catheter is passed through the nostril to the stomach for measurements during test swallows.
Preparation: Clear liquids only after midnight. No fluids 2 hours before procedure. Discontinue motility medications 24 hours before (nitroglycerin, dicyclomine, metoclopramide, etc.).
Bravo Wireless pH Monitoring
Performed at Southwest Endoscopy Center
Prolonged monitoring of lower esophageal acid levels used to confirm gastroesophageal reflux disease diagnosis when uncertain or when considering surgical treatment. A monitoring capsule is attached to the esophageal wall during endoscopy and transmits acid measurements to an external recorder for 48 hours. No nasal catheter necessary.
Preparation: Discontinue PPIs 7 days before testing. Discontinue H2 antagonists 3 days before. Clear liquids only after midnight. No fluids 2 hours before.
Proton Pump Inhibitors (PPIs)
Proton pump inhibitors are medications which reduce gastric (stomach) acid secretion. They are frequently recommended for the acute and long-term management of gastroesophageal reflux disease (GERD) and in the prevention of gastroduodenal ulcer disease secondary to nonsteroidal anti-inflammatory drugs (NSAIDs).
Common PPI Medications
- Omeprazole 20 mg (Prilosec® OTC and generic store brands) - Available without prescription, least expensive option
- Prilosec® (omeprazole) - Available as generic
- Prevacid® (lansoprazole) - Available as generic
- Prevacid 24H® - Available over-the-counter
- Aciphex® (rabeprazole)
- Protonix® (pantoprazole) - Available as generic
- Nexium® (esomeprazole)
- NEXIUM® 24HR - Available over-the-counter
- Dexilant® (dexlansoprazole)
These drugs are generally quite safe and well tolerated, effective in controlling symptoms and healing acid-related inflammation. They vary widely in cost. Decision-making about the best course of action in your case should be made in consultation with your physician.
Considerations for Long-Term Use
Based on more than 25 years of worldwide use, the following safety concerns have been identified as potentially associated with long-term PPI use:
- Possible increased risk for Clostridium difficile and other intestinal infections
- Possible increased risk for small intestinal bacterial overgrowth (SIBO)
- Possible increased risk for pneumonia
- Possible increased risk for impaired vitamin B12 absorption
- Possible increased risk for low blood magnesium level
- Possible increased risk for low iron levels
- Possible increased risk for hip, wrist and spine fractures, and osteoporosis
- Possible drug interactions (particularly with clopidogrel/Plavix)
Note: "Potentially associated" does not mean proven or that PPI use is causative of these side-effects. For most patients needing acid suppression therapy, benefits outweigh risks.
Books of Interest
For Inflammatory Bowel Disease (IBD)
A Journey to Health: Overcoming Inflammatory Bowel Disease
By Larry K. Hartsfield, PhD (Kindle Edition)
This book describes the process of healing from an auto-immune illness, specifically Inflammatory Bowel Disease. The author discusses both traditional and alternative treatments and details extensive research into illness and healing.
For Celiac Disease
Celiac Disease For Dummies
By Ian Blumer MD, Sheila Crowe MD (Paperback and Kindle)
The ultimate reference for people with celiac disease and their family members. Helps identify symptoms, explains diagnosis, outlines treatment through gluten elimination and additional nutritional measures.
For Irritable Bowel Syndrome (IBS)
IBS-Free at Last!
By Patsy Catsos
Comprehensive guide to understanding and managing IBS through dietary modifications including the low-FODMAP diet approach.
Search Engines
Doctor's Electronic Desk
These are professionally-oriented links primarily for the use of our medical staff.
Health Related Organizations and Other Sites of Interest
- American Association for the Study of Liver Diseases - Practice Guidelines
- American Cancer Society - Colorectal Cancer Screening and Surveillance
- American College of Gastroenterology
- American Gastroenterological Association
- American Society for Gastrointestinal Endoscopy
- American Society of Colon & Rectal Surgeons - Patient Education
- ARUP Laboratories
- ARUP Consult
- American Liver Foundation
- CA - A Cancer Journal for Clinicians
- Centers for Disease Control and Prevention
- CDC - Overweight and Obesity
- FDA: U.S. Food and Drug Administration
- FDA MedWatch
- eMedicine (Medscape)
- Mayo Clinic
- Mayo Medical Laboratories
- Medicare Fee Schedule
- Myriad Hereditary Cancer Testing
- National Cancer Institute
- Prometheus Labs
- Society of Gastroenterology Nurses and Associates
- UpToDate
- University of Colorado Health Sciences Center
- University of New Mexico Health Sciences Center
Clinical Guidelines and Resources
Guidelines are intended to be an educational device to provide information that may assist us in providing care to patients. Guidelines are not rules and should not be construed as establishing a legal standard of care or as encouraging, advocating, requiring, or discouraging any particular treatment. Clinical decisions in any particular case involve a complex analysis of the patient's condition and available courses of action. Therefore, clinical considerations may lead a physician to take a course of action that varies from guidelines.