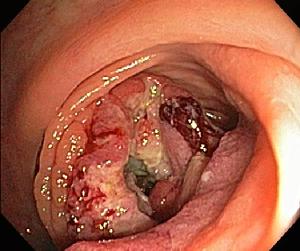
What is Colonoscopy?
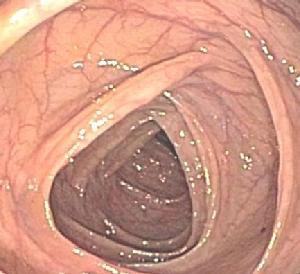
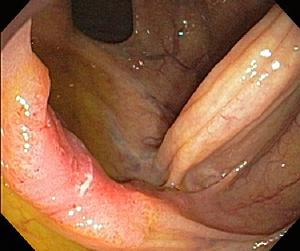
Colonoscopy is an examination of the colon, also called the large intestine, which is the last 5-6 feet of the intestinal tract, ending in the rectum. The examination is performed with a long flexible and steerable tube (colonoscope) which is about the diameter of a finger.
The tip of the tube lights the interior of the colon and projects a color image on high definition video monitors. A variety of instruments may be passed through the colonoscope, allowing the doctor to sample tissue, remove small growths, and perform a variety of treatments.
Why is Screening Important?
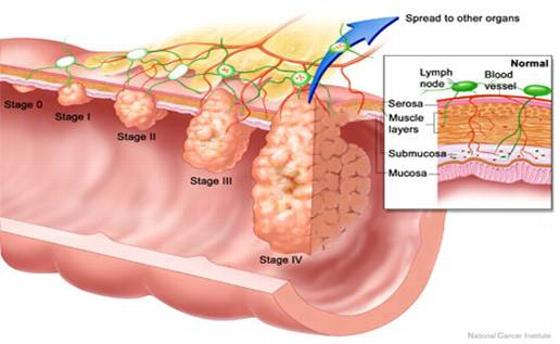
Colon cancer is the second leading cause of cancer-related death. Most people with early colon cancer feel perfectly well. Fortunately, early colon cancer can be detected by colonoscopy at early stages, before it has spread outside the colon. Early stage colon cancer is often highly curable.
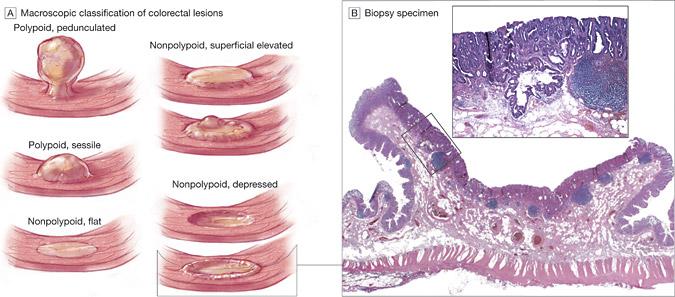
More importantly, the common growths (polyps) from which most colon cancers may slowly arise can be detected and removed during a colonoscopy, resulting in the potential prevention of colon cancer.
Experts believe that colon cancer deaths may be up to 90% preventable by regular colonoscopy, and that colon cancer itself may be up to 70% preventable.
All individuals should undergo colon cancer screening at or before the age of 45.
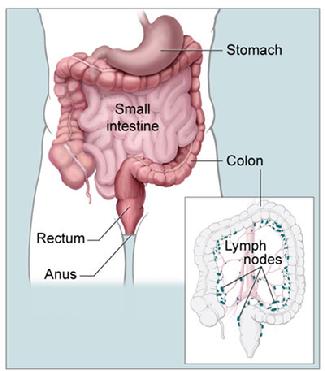
Anatomy of the colon (from the National Cancer Institute)